")
2024-01-30 ペンシルベニア州立大学(PennState)
◆この研究は、母親の空気汚染への曝露が、新生児の深刻な呼吸窮迫症状を引き起こす可能性があることを初めて示しており、これが世界中での新生児の死亡および新生児集中治療室への入院の主要原因である呼吸窮迫症の理解を深めました。
<関連情報>
- https://www.psu.edu/news/research/story/prenatal-air-pollution-exposure-linked-severe-newborn-respiratory-distress/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC10810300/
出生前の大気汚染への曝露と期産新生児の呼吸困難: MIREC前向き妊娠コホートの結果 Prenatal Exposure to Air Pollution and Respiratory Distress in Term Newborns: Results from the MIREC Prospective Pregnancy Cohort
Markey Johnson, Lauren Mazur, Mandy Fisher, William D. Fraser, Liu Sun, Perry Hystad, and Chintan K. Gandhi
Environmental Health Perspectives Published:25 January 2024
DOI:https://doi.org/10.1289/EHP12880
Abstract
Background:
Respiratory distress is the leading cause of neonatal morbidity and mortality worldwide, and prenatal exposure to air pollution is associated with adverse long-term respiratory outcomes; however, the impact of prenatal air pollution exposure on neonatal respiratory distress has not been well studied.
Objectives:
We examined associations between prenatal exposures to fine particular matter (PM2.5) and nitrogen dioxide (NO2) with respiratory distress and related neonatal outcomes.
Methods:
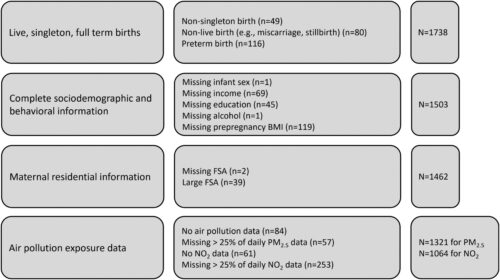
We used data from the Maternal–Infant Research on Environmental Chemicals (MIREC) Study, a prospective pregnancy cohort (n=2,001) recruited in the first trimester from 10 Canadian cities. Prenatal exposures to PM2.5 (n=1,321) and NO2 (n=1,064) were estimated using land-use regression and satellite-derived models coupled with ground-level monitoring and linked to participants based on residential location at birth. We calculated odds ratios (ORs) and 95% confidence intervals (CIs) for associations between air pollution and physician-diagnosed respiratory distress in term neonates in hierarchical logistic regression models adjusting for detailed maternal and infant covariates.
Results:
Approximately 7% of newborns experienced respiratory distress. Neonates received clinical interventions including oxygen therapy (6%), assisted ventilation (2%), and systemic antibiotics (3%). Two percent received multiple interventions and 4% were admitted to the neonatal intensive care unit (NICU). Median PM2.5 and NO2 concentrations during pregnancy were μ8.81 μg/m3 and 18.02 ppb, respectively. Prenatal exposures to air pollution were not associated with physician-diagnosed respiratory distress, oxygen therapy, or NICU admissions. However, PM2.5 exposures were strongly associated with assisted ventilation (OR per μ1-μg/m3 increase in PM2.5=1.17; 95% CI: 1.02, 1.35), multiple clinical interventions (OR per μ1-μg/m3 increase in PM2.5=1.16; 95% CI: 1.07, 1.26), and systemic antibiotics, (OR per μ1-μg/m3 increase in PM2.5=1.12; 95% CI: 1.04, 1.21). These associations were consistent across exposure periods—that is, during prepregnancy, individual trimesters, and total pregnancy—and robust to model specification. NO2 exposure was associated with administration of systemic antibiotics (OR per 1-ppb increase in NO2=1.03; 95% CI: 1.00, 1.06).
Discussion:
Prenatal exposures to PM2.5 increased the risk of severe respiratory distress among term newborns. These findings support the development and prioritization of public health and prenatal care strategies to increase awareness and minimize prenatal exposures to air pollution.
")
")