")
2026-05-07 スタンフォード大学
<関連情報>
- https://news.stanford.edu/stories/2026/05/brain-imaging-new-migraine-classifications
- https://journals.sagepub.com/doi/10.1177/03331024261433982
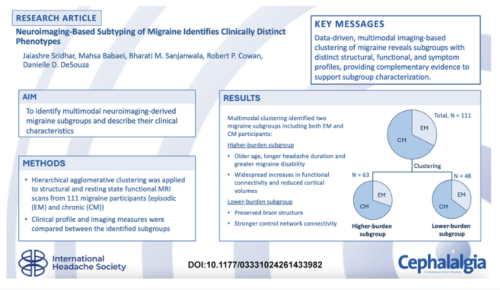
神経画像診断に基づく片頭痛のサブタイプ分類により、臨床的に異なる表現型が特定される Neuroimaging-based subtyping of migraine identifies clinically distinct phenotypes
Jaiashre Sridhar, Mahsa Babaei, […], and Danielle D. DeSouza
Cephalalgia Published:March 26, 2026
DOI:https://doi.org/10.1177/03331024261433982
Graphical abstract This is a visual representation of the abstract.
Abstract
Background
Integrating brain structure and function may help characterize neurobiological heterogeneity in migraine alongside symptom presentation.
Aim
To apply a multimodal, exploratory, data-driven approach to identify migraine subgroups using structural and functional MRI, and to describe the clinical characteristics of the resulting subgroups.
Methods
Resting-state functional connectivity (FC) across cortical and subcortical regions, along with structural measures including cortical thickness, cortical volume, and subcortical volumes, were extracted from 111 individuals with migraine (75 chronic, 36 episodic) classified according to ICHD-3 criteria. After dimensionality reduction using principal component analysis, hierarchical agglomerative clustering was applied to identify multimodal imaging-derived subgroups. For comparison, secondary unimodal clustering models were constructed using functional-only and structural-only feature sets. The optimal number of clusters was determined using silhouette coefficients, and clustering concordance across models was quantified using the Adjusted Rand Index (ARI). Group differences in clinical characteristics, FC, and cortical and subcortical structure were assessed using covariate-adjusted statistical models with false discovery rate (FDR) correction.
Results
Multimodal clustering identified two subgroups with distinct clinical and imaging profiles, Migraine Cluster 1 (M1f + s) and Migraine Cluster 2 (M2f + s). M2f + s showed older age, longer disease duration, greater migraine disability, widespread increases in cortical-subcortical FC (including Dorsal Attention, Somatomotor, and Visual networks), and reduced cortical volumes across frontal, parietal, temporal, and insular regions compared with M1f + s. This subgroup also exhibited increased connectivity relative to controls. In contrast, M1f + s showed preserved cortical structure and stronger Control-network–subcortical connectivity compared to M2f + s, and no significant functional or structural deviations from controls. Unimodal analyses revealed that Functional-only clustering aligned moderately with the multimodal cluster solution (ARI = 0.427), showing that FC was a primary determinant of the multimodal cluster structure, whereas structural-only clustering showed negligible overlap (ARI = 0.001), reflecting an orthogonal dimension of heterogeneity captured by structural variation.
Conclusion
Data-driven multimodal neuroimaging-based clustering in migraine identified two subgroups with distinct clinical and imaging patterns, highlighting heterogeneity and providing a framework for further investigation of imaging-informed characterization.
")
")