
2026-05-28 国立がん研究センター

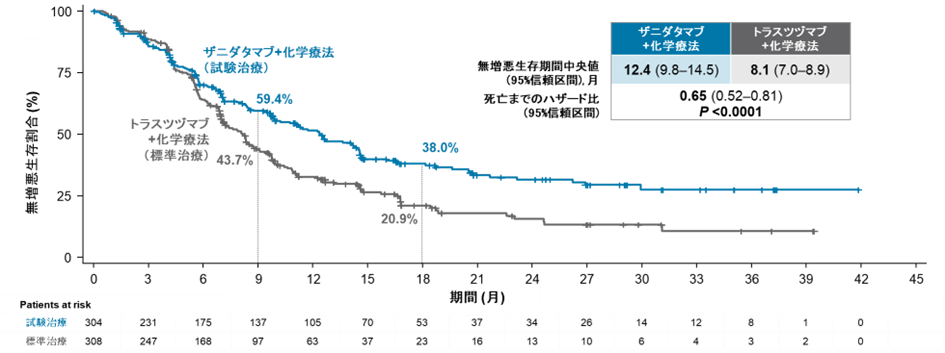
図1. 無増悪生存期間の生存曲線
<関連情報>
- https://www.ncc.go.jp/jp/information/researchtopics/2026/0528/index.html
- https://www.nejm.org/doi/full/10.1056/NEJMoa2517729
HER2陽性胃食道癌におけるザニダタマブ単独療法およびティスレリズマブ併用療法 Zanidatamab with and without Tislelizumab in HER2-Positive Gastroesophageal Cancer
Kohei Shitara, M.D., Elena Elimova, M.D., Tianshu Liu, M.D., Ph.D., Josep Tabernero, M.D., Ph.D., Keun-Wook Lee, M.D., Michael Schenker, M.D., Niall C. Tebbutt, Ph.D., M.R.C.P., F.R.A.C.P., +22 , for the HERIZON-GEA-01 Investigators
The New England Journal of Medicine Published: May 27, 2026
DOI: 10.1056/NEJMoa2517729
Abstract
Background
Zanidatamab, a dual human epidermal growth factor receptor 2 (HER2)–targeted bispecific antibody, plus chemotherapy both with and without tislelizumab (anti–programmed death 1), showed encouraging efficacy and safety as first-line therapy in phase 2 studies involving patients with HER2-positive gastroesophageal adenocarcinoma.
Methods
In an open-label, phase 3 trial, we randomly assigned, in a 1:1:1 ratio, patients with previously untreated, centrally confirmed HER2-positive advanced gastroesophageal adenocarcinoma to receive zanidatamab and tislelizumab plus chemotherapy, zanidatamab plus chemotherapy, or trastuzumab plus chemotherapy. The two primary end points were progression-free survival and overall survival.
Results
At a median follow-up of 25.9 months, progression-free survival was longer with zanidatamab–tislelizumab–chemotherapy (median among 302 patients, 12.4 months) and zanidatamab–chemotherapy (median among 304 patients, 12.4 months) than with trastuzumab–chemotherapy (median among 308 patients, 8.1 months) (hazard ratio for progression or death with zanidatamab–tislelizumab–chemotherapy, 0.63 [95% confidence interval {CI}, 0.51 to 0.78]; hazard ratio with zanidatamab–chemotherapy, 0.65 [95% CI, 0.52 to 0.81]; P<0.001 for both comparisons). Overall survival was longer with zanidatamab–tislelizumab–chemotherapy than with trastuzumab–chemotherapy (median, 26.4 vs. 19.2 months; hazard ratio for death, 0.72; 95% CI, 0.57 to 0.90; P=0.004). At this interim analysis, overall survival did not differ significantly between zanidatamab–chemotherapy (median, 24.4 months) and trastuzumab–chemotherapy (hazard ratio, 0.80; 95% CI, 0.64 to 1.01; P=0.06). The incidence of grade 3 or higher adverse events was 83.3% with zanidatamab–tislelizumab–chemotherapy, 73.8% with zanidatamab–chemotherapy, and 74.5% with trastuzumab–chemotherapy; diarrhea was the most common such event, in 24.8%, 20.0%, and 12.9% of patients, respectively.
Conclusions
Zanidatamab plus chemotherapy, both with and without tislelizumab, led to longer progression-free survival than trastuzumab plus chemotherapy among patients with HER2-positive advanced gastroesophageal adenocarcinoma. At this interim analysis, overall survival was longer with zanidatamab–tislelizumab–chemotherapy than with trastuzumab–chemotherapy; further analyses are planned to assess zanidatamab–chemotherapy. Diarrhea was a common adverse event. (Funded by Jazz Pharmaceuticals and others; HERIZON-GEA-01 ClinicalTrials.gov number, NCT05152147.)

